


Pulmonary arterial hypertension
Pulmonary arterial hypertension (PAH) is a rare condition affecting about 15 to 50 people out of every million. It is caused by very high blood pressure in the arteries that lead from the heart to the lungs, known as the pulmonary arteries. This increase in blood pressure puts strain on the heart, and will eventually cause the right side to stop working. PAH is a very serious disease, for which there is unfortunately no cure. However, there are many treatments now available that can benefit people with the condition and improve their quality of life.
What are the pulmonary arteries?
The pulmonary arteries are the blood vessels that carry blood low in oxygen from the bottom right of the heart (right ventricle) to the small arteries and capillaries in the lungs. The blood in these capillaries is then replenished with oxygen and carried back to the left side of the heart, before it is pumped around our whole body
Who gets pulmonary arterial hypertension?
Pulmonary arterial hypertension can affect people of any age, of any sex and of any race. However, it is most common in women aged between 30 and 50 years.
No information has been found, please check back soon for updates.
What are the symptoms of pulmonary arterial hypertension?
As pulmonary arterial hypertension needs to be treated as soon as possible, it is essential that it is detected very early. However, it is very difficult to identify in its early stages because its symptoms are similar to those of other heart and lung diseases. Breathlessness, especially when exercising, is the first and main symptom. It may feel as if you are not able to get enough air into your body. Other symptoms may develop as the condition gets worse.

Are there different types of pulmonary arterial hypertension?
There are a number of different causes of pulmonary arterial hypertension. These include:
- “Idiopathic” pulmonary arterial hypertension is pulmonary arterial hypertension with no obvious cause.
- “Heritable” pulmonary arterial hypertension is when the disease is shown to be caused by a problem with a gene that runs in your family. Some genes have been found to play a role in pulmonary arterial hypertension and treatment may improve and advance as more is understood about them. The most important genetic mutations associated with heritable pulmonary arterial hypertension affect the gene BMPR2, which contains the code for a protein that is found at the surface of the cells lining the pulmonary arteries.
- Associated pulmonary arterial hypertension is when the disease occurs in patients with other conditions. Examples of these include being infected with HIV, having a liver disease and having a disease associated with connective tissue (such as scleroderma or lupus). Using diet pills, cocaine or amphetamines can also increase the probability of getting pulmonary arterial hypertension.
What happens in pulmonary arterial hypertension?
Blood pressure rises in pulmonary arterial hypertension because the blood is unable to flow properly through the blood vessels. The reasons for this include:
- Narrowing of blood vessels due to muscles around the blood vessels tightening up, which is termed “vasoconstriction”.
- Changes to the shape and thickness of the blood vessel walls, because of an increase in the amount of muscle.
- Swelling of the blood vessel walls caused by inflammation.
- The formation of small blood clots within the blood vessels
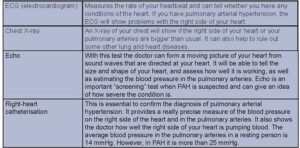
How can pulmonary arterial hypertension be diagnosed?
Doctors will perform a number of different tests to diagnose pulmonary arterial hypertension, many of which will be used to rule out other diseases with similar symptoms. Further tests may then be carried out, including lung function tests, exercise tests and blood tests.
How can pulmonary arterial hypertension be treated?
Although pulmonary arterial hypertension cannot be cured, in the past decade great improvements have been made in the understanding of the disease, which has resulted in signifi cant improvements in treatment. Treatment can now allow you to exercise longer and improve your quality of life and outcome.
Most drug treatment aim to stop or reduce the processes which block the pulmonary arteries and cause pressure to rise. Different treatments will help different people and new drugs are being developed and tested all the time. Doctors sometimes prescribe two or even three of the drugs below if the symptoms do not improve sufficiently with one drug alone.
Anticoagulants:
In the basic treatment of pulmonary arterial hypertension, you may be prescribed drugs called anticoagulants, which will reduce the risk of blood clots in your pulmonary arteries.
Calcium channel blockers:
A small group of pulmonary arterial hypertension patients will benefit from treatment with calcium channel blockers and the doctor will be able to tell this after right-heart catheterisation. Calcium channel blockers help to relax the muscles in the blood vessels, which will increase the blood and oxygen supply to the heart and reduce its workload.
Prostacyclin therapy:
Prostacyclin works by widening the arteries of the lung and preventing blood clots forming. Unfortunately, the tablet versions of prostacyclin, such as beraprost, are not very effective so the treatment has to be given in other ways: Intravenous (i.v.) prostacyclin is called epoprostenol. This can be given into the veins via a pump and is the main treatment for the most severe pulmonary arterial hypertension patients. Epoprostenol has to be given constantly in order to work effectively. As giving epoprostenol intravenously can be quite difficult, a version of the treatment has been developed which can be given under the skin (“subcutaneously”), this is called treprostinil. Recently, prostacyclin has been developed into a form that can inhaled through a nebuliser. This means that it is now easier to use and works on the lungs directly. This is called iloprost and usually needs to be taken 6 times a day. Inhaled treprostinil is currently approved in the USA.
Endothelin receptor antagonists:
Endothelin receptor antagonists are another important form of treatment. These tablets help to widen the blood vessels and reduce the build up of muscle in the vessels. Bosentan, sitaxsentan and ambrisentan are all drugs in this group.
Phosphodiesterase type 5 inhibitors and Guanylate cyclase stimulators:
Phosphodiesterase type 5 inhibitors, such as sildenafil, work by widening the arteries of the lung. Sildenafil is given by mouth three times per day. New drugs such as tadalafil are now approved in the USA and Europe. These drugs are types of targeted therapy.
Lung transplantation:
If medical therapy has not been effective, surgery to replace one or both lungs, and sometimes the heart, with healthy organs from a donor can help some patients.
Living with pulmonary arterial hypertension
A diagnosis of pulmonary arterial hypertension should not stop you from leading a full and active life, as long as it doesn’t cause you pain or problems. However, the more severe your symptoms, the less you may be able to do. There are many things that you can do to help relieve your symptoms without even taking medication:
Try to:
- Prepare nutritious meals that are low in salt.
- Control your liquid intake.
- Eat 3 meals a day.
- Sit down to eat and eat slowly.
- Brush your teeth regularly to prevent infections.
- Plan to have breaks to rest during your day.
- Prepare and organise your medication.
- Keep a medication diary, so you take your medication at the right time.
- Make sure you have extra medication; you never know when you might need it.
- Research and learn about new treatments.
- Be aware of any side-effects new medication may cause.
- Carry the contact numbers of your medical team in the event of an emergency.
- Prepare your provisions in advance if you are going away from home.
Avoid:
- High altitude.
- Pre-cooked meals.
- Smoking and alcohol.
- Becoming pregnant as this puts too much strain on your heart.
This material was compiled with the help of ERS PAH expert Prof. Marc Humbert and Dr Dermot O’Callaghan. Some images courtesy of medical illustator, Patrick J. Lynch.
This page was updated in 2024
If you want to access data on PAH in Europe, visit the Lung Facts website
Launched by the International Respiratory Coalition and using data from the Global Burden of Disease study, Lung Facts provides the latest numbers on people living with lung disease by condition and by country.
Learn more